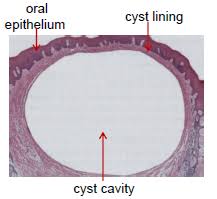
Cyst is defined as a pathological cavity may or may not be lined by epithelium and containing fluid , semi fluid or gaseous material .
Cysts are more common in the orofacial region and are the most common cause for chronic jaw swelling . They grow slowly and are usually asymptomatic . The epithelium of the cysts of oral and paraoral region is usually derived from the odontogenic apparatus and their Remnants or the epithelium entrapped at the line of fusion of various facial process during the development .
The wall of the capsule is composed of the collagenous fibrous connective tissue usually within epithelial lining and it produces various bond reserving factors for its growth and expansion .
It may occur within the bone or soft tissue . They grow by hydraulic expansion . Radiographically, they often appear radiolucency surrounded by thin radioopaque border .
TYPES OF CYSTS : TRUE CYSTS : that which is lined by epithelium e.g dentigerous cyst, radicular cyst etc. PSEUDO CYSTS: not lined by epithelium, e.g. Solitary bone cyst, Aneurismal bone cyst etc.
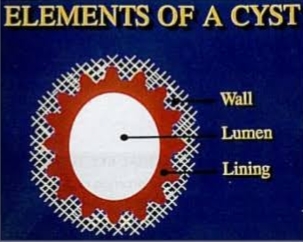
PARTS OF A CYST : Cyst has following parts: -> WALL (made of connective tissue) -> EPITHELIAL LINING. -> LUMEN OF CYST
Mechanism of cyst formation :
- Proliferation of the epithelial lining
- Food regulation within the cyst cavity
- Bone resorption
Mechanism of cyst formation Proliferation of the epithelial lining Fluid accumulation within the cyst cavity Bone resorption : Epithelial cysts A) Odontogenic cysts. 1) Developmental odontogenic cysts
- Odontogenic keratocyst
- Orthokeratinized odontogenic cyst
- Dentigerous cyst Eruption cyst
- Lateral periodontal cyst
- Glandular odontogenic cyst
- Calcifying odontogenic cyst
- Gingival cyst of newborn
- Gingival cyst of adult
2) Inflammatory odontogenic cyst
- Apical periodontal cyst
- Inflammatory collateral cyst
- Paradental cyst
- Buccal bifurcation cyst
B) non odontogenic cysts 1) developmental non odontogenic cysts
- Nasopalatine duct cyst
- Median palatal cyst
- Globulomaxillary cyst
- Median mandibular cyst
- Palatal cysts of neonate
- Nasolabial cyst
- Thyroglossal duct cyst
- Oral lymphoepithelial cyst Epidermoid cyst
- Dermoid cyst
2) inflammatory non odontogenic cysts
- Salivary cysts
- Mucous extravasation cyst
- Ranula
- Mucous retention cyst
- Antral cysts
- Retention cyst of maxillary sinus
- Surgical ciliated cyst of maxilla
- Traumatic bone cyst
- Aneurysmal bone cyst
- Parasitic cysts
C) miscellaneous cyst
- Heterotopic oral gastrointestinal cyst
- Stafne bone cyst
- Anterior lingual depression
1. Odontogenic cysts
Developmental :
Intraosseous :
– Odontogenic keratocyst – Orthokeratinized odontogenic cyst -Dentigerous cyst – Lateral periodontal cyst – Glandular odontogenic cyst – Calcifying odontogenic cyst
Extraosseous :
– Eruption cyst
-Botryoid odontogenic cyst
-Gingival cyst of newborn -Gingival cyst of adult
Inflammatory :
– Apical periodontal cyst – Inflammatory collateral cyst/inflammatory periodontal cyst – Residual cyst -Paradental cyst -Buccal bifurcation cyst
Cysts associated with the maxillary antrum are
1. Mucocele
2. Retention cyst
3. Pseudocyst
4. Postoperative maxillary cyst
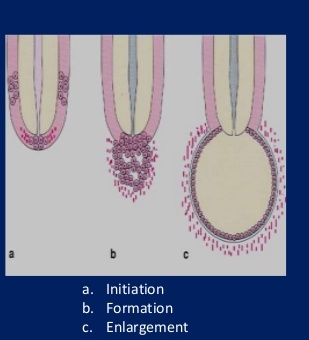
PATHOGENESIS THREE STAGES
1. Cyst initiation
2. Formation 3. Cyst enlargement or expansion
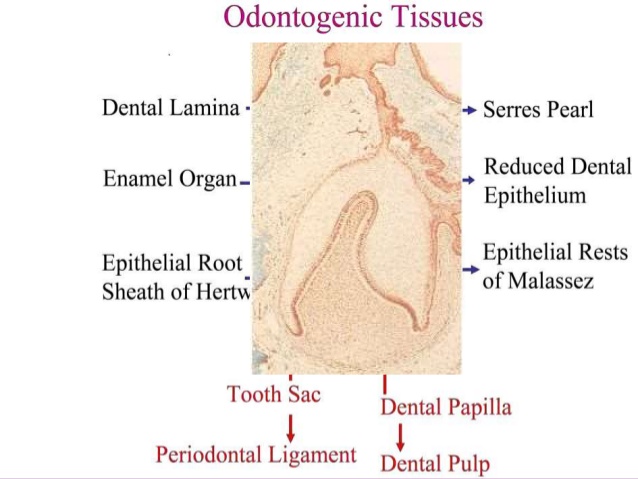
Odontogenic cyst :
The odontogenic cysts are derived from epithelium associated with the development of the dental apparatus . The type of epithelium can vary with most lesions on having stratified squamous but some developmental or fissural cyst in the maxilla may have respiratory epithelium .
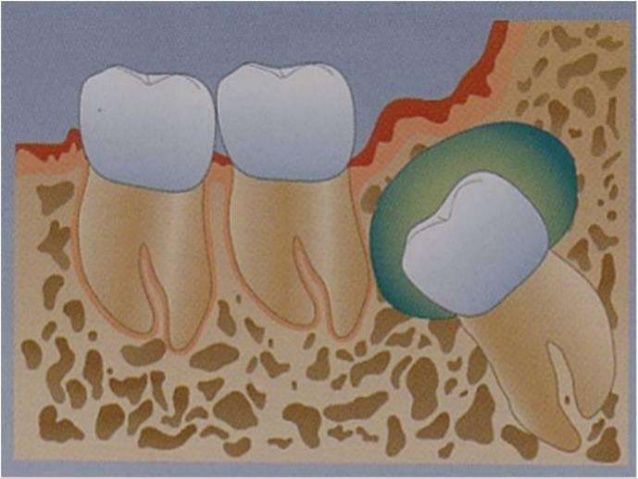
Dentigerous cyst / follicular cyst :
Definition: The dentigerous cyst is defined as a cyst that originates by the separation of the follicle from around the crown of an unerupted tooth.
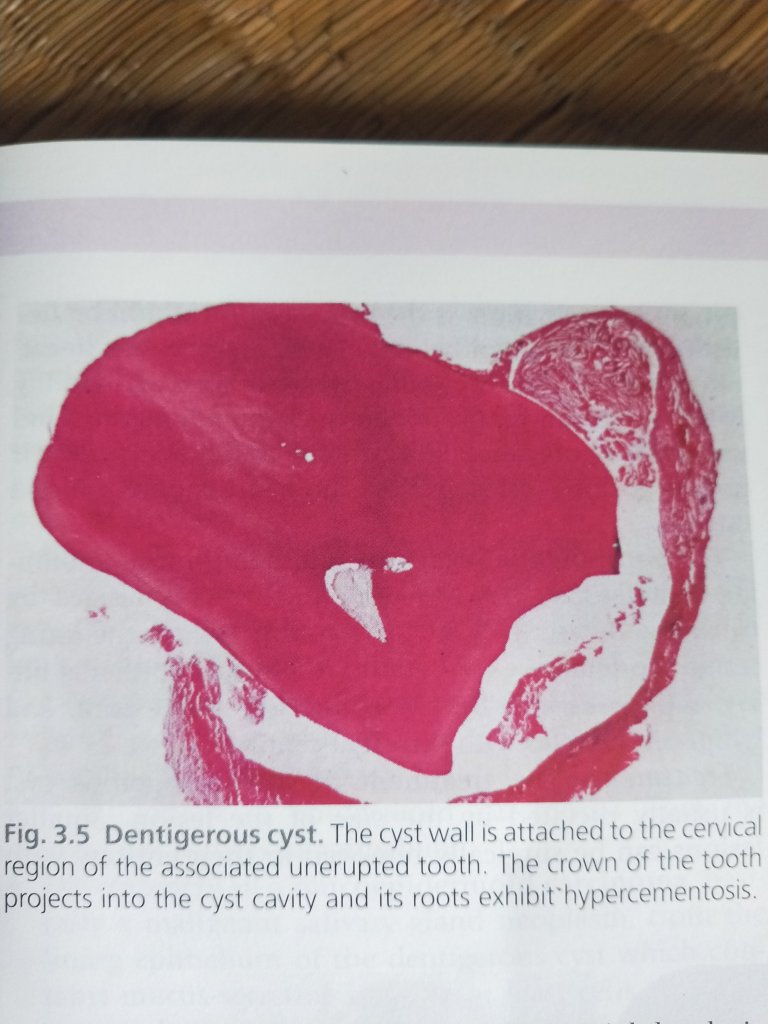
The dentigerous cyst encloses the crown of an unerupted tooth and is attached to the tooth at the cementoenamel junction .
• The pathogenesis of this cyst is uncertain, but apparently it develops by accumulation of fluid between the reduced enamel epithelium (REE) and the tooth crown.
It is estimated to be about 20% of all jaw cysts. It is estimated that about 10% of impacted teeth have form a dentigerous cyst . The dentigerous cyst nearly always involves or is associated with the crown of a normal permanent tooth .
Clinical features :
- AGE : 1st to 3rd decades.
- GENDER : more frequently in males than in females.
- SITE :
- 2/3rd of follicular cyst associated with unerupted mandibular teeth, primarily III molar.
- Maxillary canine
- Mandibular premolar
- Maxillary 3rd Molar
- Supernumerary tooth also can be involved
- Dentigerous cysts have the potential, to attain a large size, often it is the pronounced facial asymmetry .
- Teeth displacement
- Root resorptions
- Pain may be a presenting symptom, if secondary infection occures.
- Eggshell crackling, in large cysts
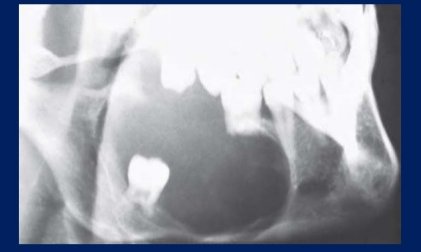
Radiographic features :
- generally reveals a unilocular radiolucency associated with crowns of unerupted teeth ( multilocular effect can be seen, in large cysts due to bony trabeculations).
- Cysts have a well defined sclerotic margin, unless when they are infected then the margins are poorly defined.As compared to the other jaw cysts,
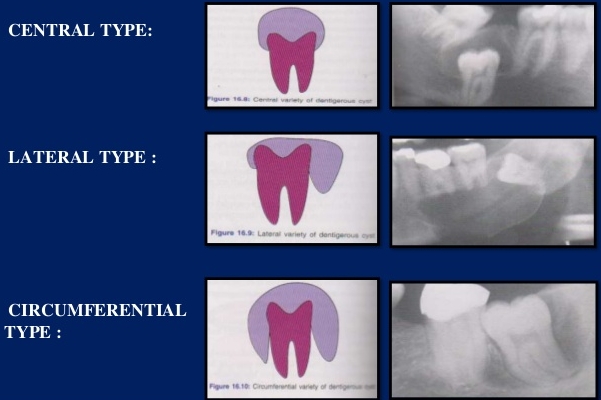
- The dental follicle may expand around the unerupted or impacted tooth in three variations : (a) circumferential (b) lateral (c) central or coronal
Cystic contents (aspirate): The cystic contents consist of clear yellowish fluid, in which cholesterol crystals may be present, and if the cyst infected it may show a purulent material .

HISTOLOGICAL FEATURES
A. NON INFLAMMED TYPE:
- Lining derived from reduced dental epithelium, consists of 2-4 cell layers of non keratinized epithelium, without rete ridges.
- Wall composed of thin fibrous connective tissue appearing immature, as it is derived from the dental papilla.
B. INFLAMMATORY TYPE :
- Lining shows varying degrees of hyperplasia with rete ridges and occasionally even keratinization.
- Wall is composed of mature connective tissue which shows infiltration by chronic inflammatory cells.
- Focal areas of mucous cells can be seen in the lining. Small odontogenic epithelial islands can be seen in the wall.
DIFFERENTIAL DIAGNOSIS: Although it presents a unique feature, yet some lesions must be considered in its differential diagnosis : 1. Unicystic ameloblastoma 2. Adenomatoid odontogenic tumor.

COMPLICATIONS :
1. Recurrence due to incomplete surgical removal.
2. Development of ameloblastoma either from lining epithelium or from odontogenic islands in the connective tissue wall.
3. Development of squamous cell carcinoma from same two sources.
4.Development of mucoepidermoid carcinoma from mucus secreting cells in the lining.
Treatment :
> Marsupialization ; It is indicated in children if the cyst is very large in size and the involved tooth/teeth are to be maintained.
> Enucleation with or without packing of defect when the possibility of the tooth erupting is low.
Behavior and prognosis : Recurrence rate is low . It is widely believed that ameloblastomas frequently arise in dentigerous cysts so lining of the cyst should be examined histopathologically . KERATOCYST
ODONTOGENIC KERATOCYST :
> The term OKC was first coined by Philisen in 1956.
> Its characteristic features first described by Pindborg & Hansen in 1963.
> Definition – According to WHO it is a benign uni or multicystic intraosseous tumor of odontogenic origin (dental lamina and its remnant) with characteristic lining of parakeratinised stratified squamous epithelium & potential for aggressive and infiltrative behavior.
> the lesion is named keratosis because the lining epithelium produces so much keratin that almost fills the cyst lumen .
> Keratin produced by cystic lining.
> Parakeratine lined cystic lesion within bone.
> Rare distinctive developmental odontogenic cyst from the dental lamina.
> Cyst containing clear fluid & cheesy material resembling keratin debris .
• The odontogenic keratocyst is a distinctive form of developmental odontogenic cyst that deserves special consideration because of its specific histopathologic features and clinical behavior.
• There is general agreement that the odontogenic keratocyst arises from cell rests of the dental lamina.
• This cyst shows a different growth mechanism and biologic behavior from the more common dentigerous cyst and radicular cyst.
• Growth may be related to unknown factors inherent in the epithelium itself or enzymatic activity in the fibrous wall.
• Several investigators suggest that odontogenic keratocysts be regarded as benign cystic neoplasms rather than cysts .
Pathology :
The primordial cysts are thin walled and are lined by a regular keratinized stratified squamous epithelium. The keratin formed by the epithelium is seen in two variants,
> parakeratinized – in which there is persistence of the nuclei
> orthokeratinized – in which the nuclei are absent.
Clinically, the parakeratinized variant appears to have a much higher incidence of recurrence .
COMPLICATIONS IN OKC : 1. Malignant transformation of cyst lining rare, but has been reported. 2. Recurrence high rate of recurrence.
possible reasons reported for high recurrence rate –
- Scolloped margins
- Presence of daughter cysts
- Cystic lining is very thin and fragile, portions of which may be left behind
- Epithelial lining of keratocysts have an intrinsic growth potential
- new cysts can arise from basal cells of the oral mucosa
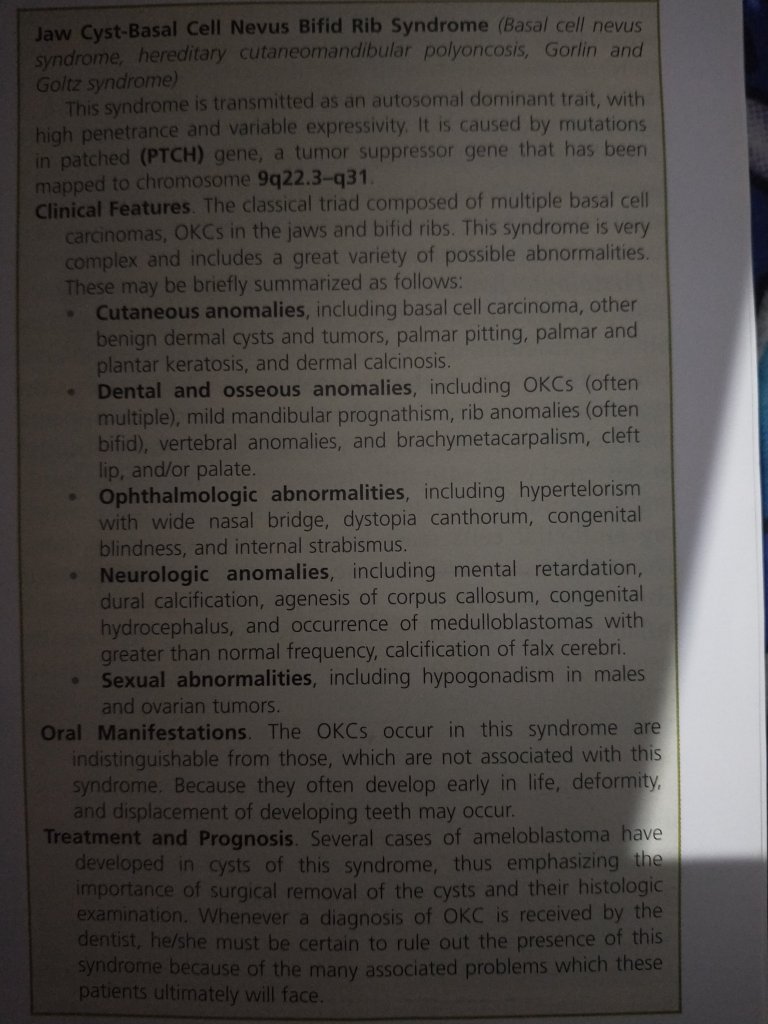
- Patients with nevoid basal cell carcinoma syndrome (Gorlin- Goltz syndrome) have a particular tendency to form multiple keratocysts with other manifestations in different parts of the body (Multiple basal-cell carcinomas of the skin, rib and vertebrae anomalies, intracranial calcifications, frontal bossing, hypertelorism , and mandibular prognathism .palmar and plantar pitting ).
Other reasons are –
1. Thin, fragile lining is very difficult to remove completely.
2. New cysts develop from satellite cysts left behind.
3. Some cysts may be left behind in cases of Gorlin Gotz syndrome.
4. New cysts can also develop from basal cells of overlying oral epithelium, especially in ramus 3rd molar region .
CLINICAL FEATURES
> Swelling with or without pain
> Discharge
> Displacement of teeth
> Occasionally paresthesia of lower lip.
> Expansion of the cyst is very minimal in the initial stage.
> Expansion of buccal cortical plate 30% in maxilla (third molar area followed by the cuspid region )and 50% in mandible ( occurring in the Ramus third molar area followed by the first and second molar areas and the anterior mandible ) .
AGE –
Peak frequency in the 2nd and 3rd decades.
GENDER : more frequently in males than in females.
SITE : The mandible > maxilla
Develop pathological fractures.
In many instances – free of symptoms until the cysts have reached a large size, involving the maxillary sinus and the entire ascending ramus, including the condylar and coronoid processes.
OKC tends to extend in the medullary cavity and clinically observable expansion of the bone occurs late.
RADIOGRAPHIC FEATURES : OKC demonstrate a well-defined radiolucent area with smooth and often corticated margins.
• Large lesions, particularly in the posterior body and ascending ramus of the mandible, may appear multilocular An unerupted tooth is involved in the lesion ; in such instances, the radiographic features suggest the diagnosis of dentigerous cyst .
Histopathology :
• Uniform layer of stratified squamous epithelium, usually 5-8 cells in thickness.
• The basal layer exhibits a characteristic palisaded pattern with polarized and intensely stained nuclei of uniform diameter.
•The luminal epithelial cells are parakeratinized and produce an uneven or corrugated profile.
- Flat epithelium and connective tissue interface absence of rete ridge.
- Basal cell layer has columnar / cuboidal cells with reversely polarized nuclei, imparting a “picket fence” or “tombstone” appearance.
- Small satellite cysts, cords, or islands of odontogenic epithelium may be seen within the fibrous wall.
- Unilocular or multilocular radiolucency with well defined border and some times associated with sclerotic margin.
- Usually extend in anteroposterior direction.
- Large mandibular cysts deflect the neurovascular bundle into an abnormal position.
- Neuropraxia may associated with infected cyst .

Treatment of keratocyst :
> Treatment should always be based on proper clinical assessment, accurate diagnosis and appropriate tests of the cystic aspirate.
Treatment options for keratocyst : • 1. Total enucleation and primary closer. The surgical procedure for treatment of a cyst with enucleation includes the following steps: 1. Reflection of a mucoperiosteal flap. 2. Removal of bone and exposure of part of the cyst. 3. Enucleation of the cystic sac. Care of the wound and suturing.
• 2. Enucleation with chemical fixation. recommended use of Cornoy’s solution after enucleation to destroy the daughter cysts and remnant lining. The Cornoy’s solution acts as chemo-cauterization to prevent recurrence.
•3. Marsupialization (usually not enough in keratocyst due to high recurrence rate) .
Marsupialization – the surgical opening of the (KCOT) cavity and a creation of a marsupial- like pouch, so that the cavity is in contact with outside for an extended period.
• 4. Resection.(in case of multiple recurrence)
> Surgical removal of segment of mandible or maxilla without maintaining the continuity of the bone >Recurrence rate 0%
• 5. Wide (local) surgical excision to prevent the recurrence .
It is also essential that patients with an OKC, especially if multiple, be evaluated medically to rule out the possibility of the jaw cyst-basal cell nevus-bifid rib syndrome .

Useful 👍
LikeLike
Thank you 😊 Mam
LikeLike
Great info.
LikeLike
Thank you 😊 Mam
LikeLike
Nice information
LikeLike
Thank you sir 😌
LikeLike
Very Useful
LikeLike
Thank you ☺️ Mam
LikeLike
Helpful😊
LikeLike
Thank you 😊 Mam
LikeLike