Introduction
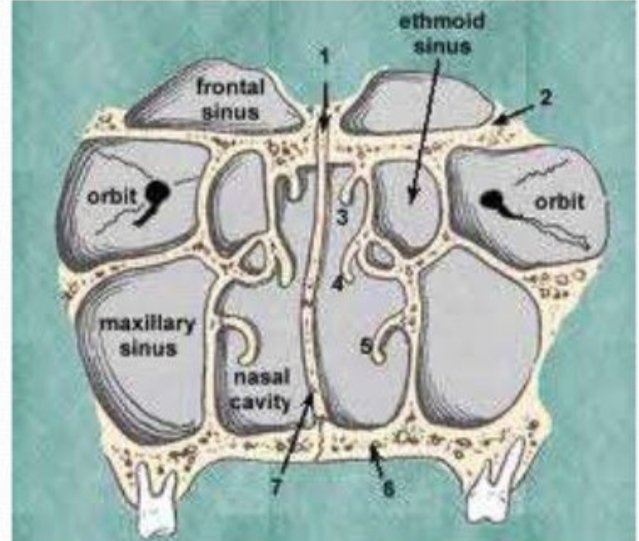
• Paranasal sinus are air containing bony spaces around the nasal cavity.
• There are 4 pairs of paranasal sinuses(bilaterally).
I. Maxillary
II. Frontal
III. Ethmoidal
IV. Sphenoidal
V. It is is also called as Antrum of Highmore.
* LARGEST paranasal sinus.
Discovery
• The maxillary sinus was first discovered and illustrated by Leonardo da vinci, but the earliest attribution of significance was given by NATHANIEL HIGHMORE.
• The British surgeon and anatomist who described it in detail in the year 1651.
Definition
• The maxillary sinus is the pneumatic space that is lodged inside the body of the maxilla and that communicates with the environment by way of the middle nasal meatus and the nasal vestibule.
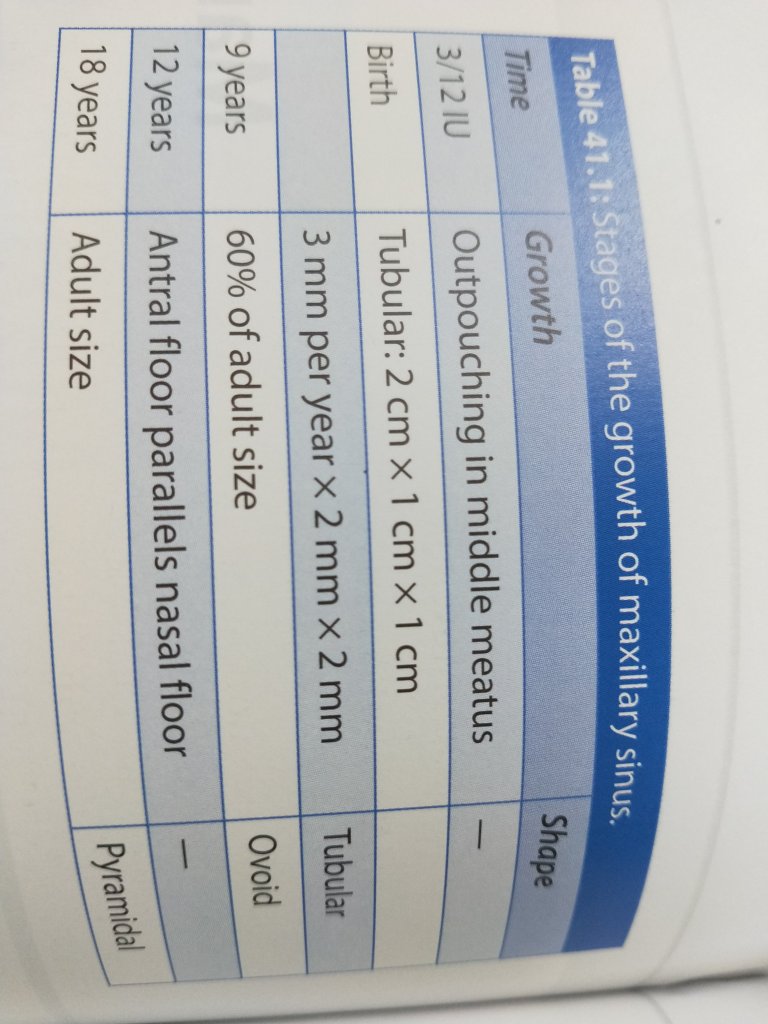
Development of sinus
• At the birth- Tubular.
• At the childhood-Ovoid.
• In the adult- Pyramidal.
Anatomy
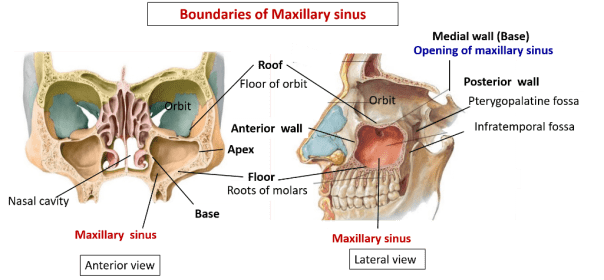
• Pyramidal shaped cavity with in the body of maxilla.
• Boundaries: Apex- zygomatic process of maxilla.
• Base- nasal surface of maxilla. • Roof-orbital surface of maxilla.
• Floor- alveolar process of maxilla.
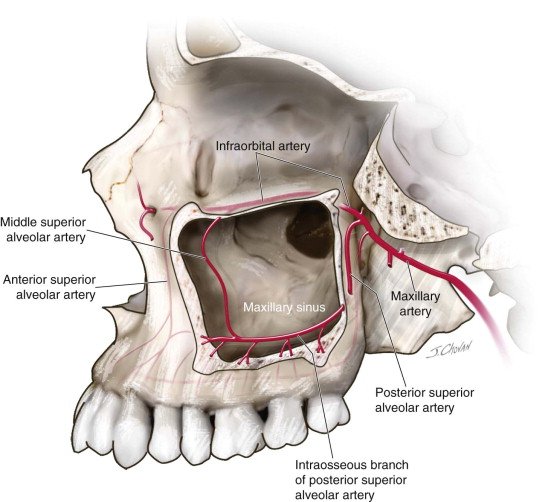
• Anterior wall is related to infra-orbital plexus of nerves and vessels and origin of muscles of upper lip.
• Posterior wall is pierced by post. Superior alveolar nerve and vessels.
Anatomy
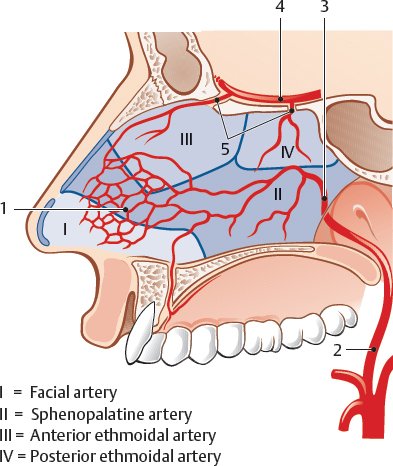
• Arterial supply-
1. Facial artery 2. Maxillary artery 3. Infra-orbital artery 4. Greater palatine artery.
Anatomy
• Venous drainage-
Anteriorly- sphenopalatine vein
Posteriorly- pterygoid venous plexus drains into facial vein
Pterygoid plexus communicates with the cavernous sinus by emissary veins.
Anatomy
• Nerve supply
1. Anterior superior alveolar nerve. 2. Middle superior alveolar nerve 3. Posterior superior alveolar nerve 4. Infra-orbital nerve 5. Greater palatine.
Anatomy
• Lymph drainage-
1. Submandibular lymph nodes. 2. Deep cervical lymph node. 3. Retro pharyngeal lymph node
Microscopic features
• 3 layers surround the space of the maxillary sinus.
1. Epithelial layer 2. Basal layer 3. Sub-epithelial layers including periostium.
Functions
1. Warming of inspired air. 2. Humidification of dry air. 3. Lightening of skull weight. 4. Resonance of voice. 5. Filters debris. 6. Accessory olfactory organ. 7. Protects skull from mechanical shock. 8. Production of bactericidal lysozyme.
Embryology (Growth of Maxillary Sinus)-
In early stages, maxillary sinus is high in maxilla. Later gradually grows downward, by a process of pneumatization . The expansion of the sinuses normally ceases after eruption of permanent teeth. However, occasionally, the sinuses pneumatize further, after removal of one or more of maxillary posterior teeth, and extend into the residual alveolar process. In adults, the apices of the posterior teeth may extend into the sinus cavity.
Physiology
The sinuses are lined by respiratory epithelium; namely, the mucus secreting; pseudostratified, ciliated, columnar epithelium. It is also known as schneiderian membrane. The mucociliary mechanism is useful means for removal of particulate matter, bacteria, etc. The cilia moves the mucus and other debris towards the ostium, and subsequently discharged in the middle meatus.
They create air padding to provide thermal insulation to the important tissue mentioned above.
Diagnostic evaluation of maxillary sinus.
Detailed medical & dental history.
Clinical examination.
Inspection Palpation Percussion Transillumination Radiographs.
Ultrasound, CT scan, MRI. Endoscopy.
Palpation –
• Tapping of lateral wall of sinus over prominence of cheek bone and palpation intra-orally on lateral surface of maxilla between canine fossa and zygomatic buttress.
Transillumination –
• It is done by placing a bright flash light or fiber optic light against the mucosa on the palatal or facial surface of the sinus and observing the transmission of light through the sinus in the darkroom.
Radiographs
Intra-oral – • Periapical • Occlusal • Lateral
Extraoral – • Panoramic • Waters view • Submentovertex • PA view
CT Scan &MRI –
• Provides multiple sections at different planes • High resolution • Non-invasive techniques
Ultrasound –
• Introduced by LANDMAN in 1986 • Non-invasive • Safe Quick • Ultrasound waves are generated by probe.
Endoscope –
• Allows direct visualization in inaccessible areas, such as maxillary moral roots that are behind distobuccal root of maxillary 1st molar.
Pathology
• Developmental anomalies. • Infections (sinusitis). • Dental implications of maxillary sinus. • Oro-antral fistula. • Toothache of maxillary sinus origin. • Associated cysts. • Associated tumours.
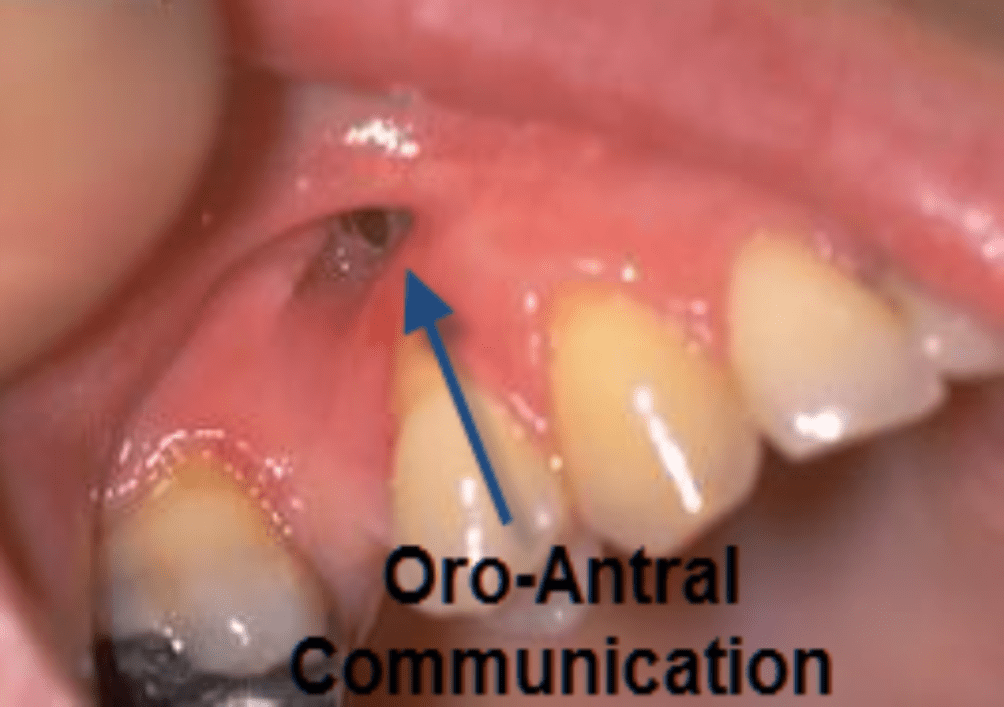
Oro-Antral fistula
• Invasion of the maxillary sinus and establishment of direct communication with the oral cavity is referred to as an oro-antral fistula.
Fistula
• It is a biological tract that connect an anatomical cavity with the external surface or other anatomical cavity. It is always lines by stratified squamous epithelium and the potency of the tract is preserved until epithelial cells scraped off.
Factors – influencing creation of oro-antral fistula.
• Hypercemntosis. • Density of alveolar bone and thickness of sinus. • Size if sinus. • Rough extraction. Apical pathosis. • Attached granulomas. • Periodontal disease that may erode the sinus floor. • Presence of cyst or tumor.
Sings & Symptoms
• Antral floor fracture. • Fracture of alveolar process or tuberosity. • Evidence of air stream passing from nostril. Change in speech tone and resonance. • Bubbling of blod from the socket or nostril.
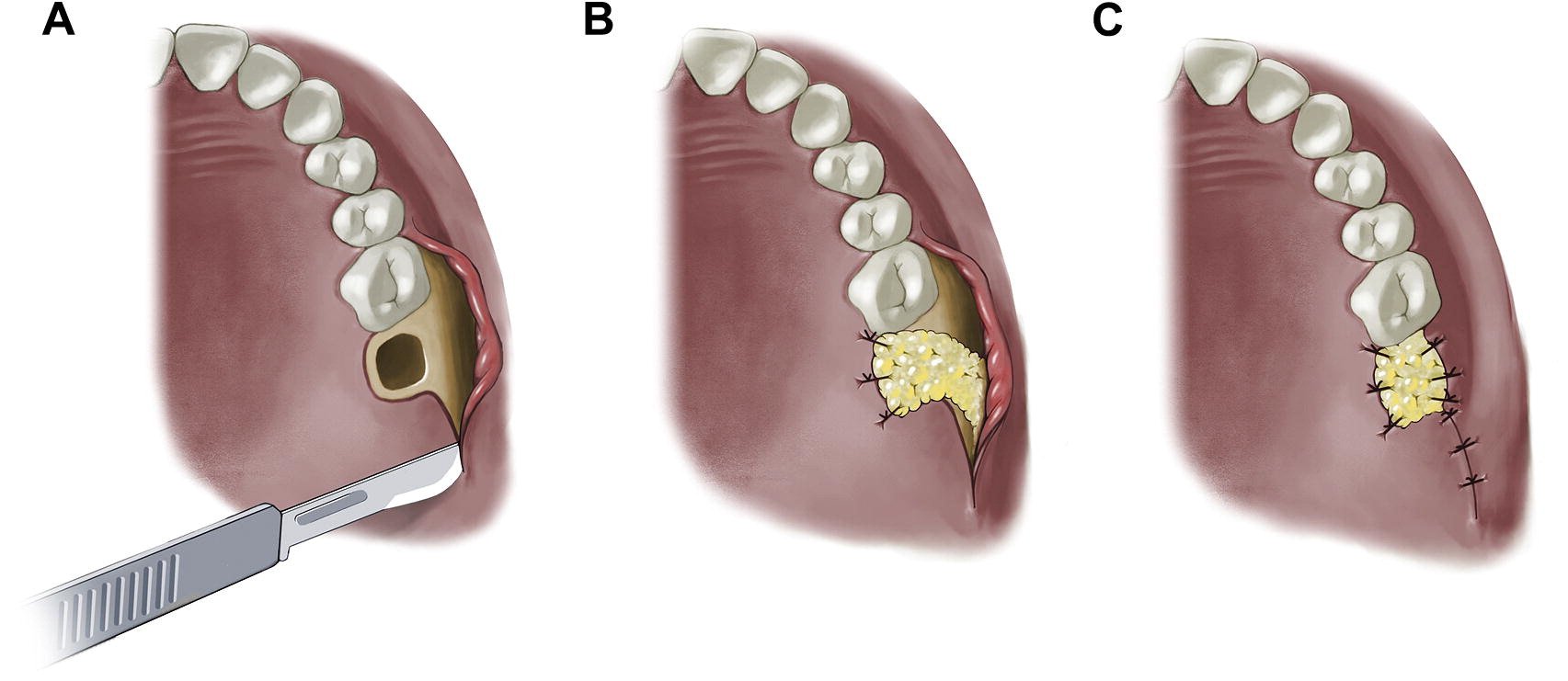
Treatment Flap surgeries.
1. Buccal flap. 2. Palatel flap. 3. Or combination.

Helpful 👍
LikeLike