Diabetes mellitus (DM) is a metabolic disorder characterized
by hyperglycemia due to absolute or relative deficiency of
insulin.
Diabetes is a metabolic dis- order whose exact cause remains still unknown. There is a disturbance of carbohydrate metabolism proper utilization with the result that there is hyper- glycaemia. The normal levels of blood sugar are dependent on the adequate amounts of insulin be- ing secreted in the body. Insulin is produced in the body by the beta cells of the islets of Langerhans of pancreas. Main stimu- lus for release of insulin is hyperglycaemia caused and there is deficiency of insulin required for its by ingestion of carbohydrates, hyperamino-acidae- mia dde to protein ingestion hormones like gluca- gon. gastrin, secretin pancreozymin and binding of insulin molecules to insulin receptors. Insulin fa- vours the entry of glucose into the liver, into mus- cles as glycogen and builds up adipose tissue by converting glucose into fat. Insulin secretion decreases with age since by the process of ageing the number of beta cells are lost by degeneration. Normally these cetls regenerate but in diabetes there is inherent defect in the regenera- tion of cells. Though mechanisms like lack of syn- thesis and release of insulin are operative in major- itý of diabetics yet other factors like defect in the transport mechanism of insulin, DNA sequence cod- ing insulin receptors and degenration of insulin on the cell surface may be operative.
Obese people are more prone to suffer from diabetes probably because obesity imposes a strain on the islets of langerhans and there is a rela- tive deficiency of insulin. Obese also show a rela- tive resistance to insulin due to reduction in the number of insulin receptors on target cells.
Exercise – Lack of physical effort and exercise promotes obesity and indirectly predisposes to dia- betes. Physical effort and leading an active life goes a long way in keeping one self trim and helps in the proper utilization of body glucose and maintains a homeostatic balance. Diet – Excessive intake of carbohydrates and re- fined sugars produces strain on the pancreas and this combined with sedentary occupation goes a long way in predisposing to diabetes.
Parity – Women with repeated pregnancies are more liable to develop diabetes since too many preg- nancies are a strain on the carbohydrate metabo- lism and often there is hormonal imbalance. Parity is an important predisposing factor in the causation of diabetes in middle aged women hav- ing more than seven children. All these factors go a long way in understanding the primary form of diabetes especially if one keeps in mind the faulty gene, over eating, obesity, lack of physical effort, racial, social and environmental factors in addition to hormonal imbalance.
Classification of diabetes mellitus
1. Type 1 diabetes mellitus
A. Immune mediated
B. Idiopathic
2. Type 2 diabetes mellitus
3. Other specific types:
a. Genetic defects of beta cell function
b. Genetic defects in insulin action
c. Diseases of pancreas: pancreatitis, neoplasia,
hemochromatosis, pancreatectomy
d. Endocrinopathies: acromegaly, Cushing’s syndrome,
hyperthyroidism pheochromocytoma, glucagonoma
e. Drugs and chemicals: thiazides, corticosteroids,
phenytoin, thyroid hormone
f. Infections: congenital rubella, coxsackie, cytomegalo
virus
g. Uncommon forms of immunemediated diabetes
h. Genetic syndromes: Down’s syndrome,
Klinefelter’s syndrome, Turner’s syndrome
4. Gestational diabetes mellitus
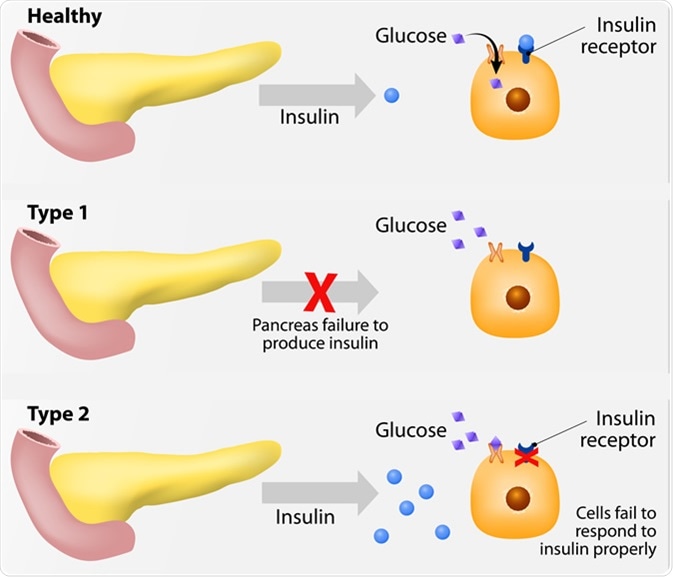
TYPE 1 DM ( INSULIN DEPENDENT DIABETES MELLITUS ) : commonly in children and young
adults . Pancreatic beta cells fail to respond to insulinogenic
stimuli. There is also role of islet cell antibodies, insulin auto antibodies and auto immune mechanism. Most of these diabetics are under- weight, undernourished and their symptoms are se- vere. Presence of ketone bodies in the urine is quite common In such diabetics since their diabetes is brittle. These patients are more liable to develop complications. They are sensitive to insulin but do not respond to oral antidiabetic drugs. Type I A diabetes is a T-cell mediated autoimmune disease
and may be associated with other autoimmune diseases like
thyroid disease, Addison’s disease, vitiligo and pernicious
anemia .Possible triggers are viral infections (coxsackie, rubella),
bovine milk protein and nitrosuria compounds. Pancreatic islets are infiltrated with lymphocytes. Risk of developing DM is increased 10
fold in the relatives of type 1 DM patients.
TYPE 2 DM ( non insulin dependent diabetes mellitus ) : it was in adult generally above the age of 40 years (mostly obese ) . It is polygenic and multifactorial in origin involving
genetic and environmental factors. Three basic
pathophysiological abnormalities : a. Impaired insulin secretion
b. Insulin resistance (inability of insulin to act on target
tissues mainly liver and muscles)
c. Increased hepatic glucose production . Patients have little tendency to ketosis and are relatively insensitive to insulin. Plasma insulin levels are either normal or raised. Genetic factors appear to play a major role in this form of diabetes and transmission is suggested to be due to an autosomal dominant trait. There are two main defects i.e. abnormal insulin secretion and insulin resistance to action in target organs. Many obese or overweight diabetics secrete large quantities of insulin but this insulin is ineffective at cellular level. There are insulin receptors on the cell wall and insulin attaches itself to these receptors before exerting its biochemical effect. Lack of adequate number of insulin receptors on the cell sur- face may be responsible for the induction of diabetes. Weight loss in such persons is known to result in increase in receptors and benefit such diabetics. In addition to the above two classical types of diabetes there is pancreatic diabetes, J type diabetes and young ketones resistant diabetes. There is hyperglycemia but
endogenous insulin prevents the development of ketoacidosis.
Hyperglycemia worsens insulin resistance and beta cell
response to glucose (glucose toxicity) and both improve
when glucose is normalized with the treatment.
Many biologic products are secreted by adipocytes that
modulate insulin secretion, insulin action, and body weight.
Leptin and adiponectin improve insulin sensitivity while tumor
necrosis factor alpha and resistin interfere with insulin action.
CLINICAL FEATURES : These are variable and may range from and due to acute complication like diabetic coma . Diabetes should be suspected if a patient has increased hunger (polyphagia ) thirst ( polydypsia ) and polyuria . Other symptoms are tiredness, fatigue, and irritability.
Blurring of vision, frequent infections, and slow healing of
wounds may also be present. The infections include bacterial
and fungal infections of skin and genitalia. The patients with type 2 DM may present with the
features of chronic neurological, cardiovascular, ophthalmic
and renal complications . Chronic skin infections,
generalized pruritus and fungal vaginitis are common. Females who have unexplained fetal loss or deliver large
babies should be screened for DM.
The patients may present with acute complications such
as diabetic ketoacidosis (DKA), hyperglycemic hyperosmolar
state (HSS) or features of chronic complications.
Complications of diabetes : Complications of diabetes may be acute in the form of diabetic coma which is a medical emergency and requires immediate management or chronic complications which are present in majority of patients. Diabetics are six to eight times more liable to heart disease than non- diabetics. Diabetes effects blood vessels both large (macrovascular disease) and small vessels particu- larly the capillaries (microvascular disease or microangiopathy). Macrovascular disease in the form of premature atherosclerosis accounts for much of morbidity in maturity onset diabetes. There is characteristic thickening of the intimal layer and li- pid material gets deposited in the intimal plaques. Aorta, carotids coronary arteries and vessels of the limbs are commonly involved. In microangiopathy there is thickening of başement membrane with hypertrophy and hyperplasia of the lining cells pro- gressing to vascular occlusion. In fact coronary heart disease is the major cause of death in diabetics after the age of 40. Ischaemic heart dis- ease in the form of myocardial infarction, angina pectoris is very common in diabetics. Again pain- less myocardial infarction explained on the basis of autonomic diabetic neuropathy or involvement of coronary vessels is common in diabetics as com- pared to non-diabetics. Diabetic cardiomyopathy, cerebrovascular accidents and hypertension are other vascular complications. gangrene of the foot occurs as a result of neuropathy microangiopathy and secondary infection. Renal lesions: Urinary tract infections, Glomerulosclerosis . GI manifestation – gastritis ( acute or chronic ) diarrhoea , nocturnal diarrhoea , paralytic ileus cholecystitis . Eye – diabetic retinopathy .
Investigations :
Urine Test :
The urine is tested for the presence of glucose, ketones,
and protein. Presence of albumin (>30 mg/dL) in the urine
suggests nephropathy.
BLOOD TEST:
The plasma glucose tests are performed for the diagnosis
of DM (see above). The fasting plasma glucose is done
after overnight fast (at least 8 hours fast). The random test
is defined as without regard to time since the last meal.
Oral glucose tolerance test (OGTT) is performed by
giving 75 g glucose dissolved in water and measuring plasma
glucose after 2 hours. The persons should be on unrestricted
carbohydrate diet for 3 days before the test.
The random blood sugar is performed first. If the
random plasma glucose level is increased but not diagnostic
(<200 mg/dL), fasting plasma glucose is measured. When
the fasting plasma glucose level is <126 mg/dL, OGTT is
performed.
The criteria for the diagnosis of DM in pregnancy
(gestational diabetes) are different and more stringent .
Serum Fructosamine Measurement :
Serum fructosamine is formed by non-enzymatic glycation
of serum proteins, mainly albumin. Its level reflects the
glycemic control for the preceding 2 weeks. This is
particularly useful for the assessment of the glycemic control
in diabetic women.
Self Monitoring of Blood Glucose :
Glucometers are available for the measurement of capillary
blood glucose. The test can be performed by the patients
themselves at home.
Continuous Blood Glucose Monitoring System :
The blood glucose can be monitored continuously
throughout 72 hours with the help of a subcutaneously placed
sensor. This is useful in the detection of asymptomatic
hypoglycemia.
Other Tests :
Serum lipids are routinely measured. Patients with type 2
DM may have dyslipidemia characterized by high
triglycerides, low HDL cholesterol, and presence of small
dense LDL particles. These patients are more susceptible to
atherosclerosis. Type 1 diabetics have raised triglycerides and LDL
cholesterol but normal HDL cholesterol.
Blood urea, serum creatinine, electrolytes, liver function
tests are also performed.
Management of Diabetes :
This includes diet modification, exercise, education and
medications.
Ideal goals of the glycemic control in patients with DM
are as follows. However, these goals are individualized.
1. Average preprandial glucose values 90-130 mg/dL
2. Bedtime glucose value of 100-140 mg/dL
3. Peak postprandial glucose less than 180 mg/dL
4. The level of HbA1C less than 7%
The management of patients with DM includes:
a. Glycemic control
b. Treatment of associated conditions like hyper-
tension, dyslipidemia, obesity and cardiovascular
disease
c. Detection and management of diabetes related
complications.
Complications of diabetes mellitus : Acute complications 1. Diabetic coma. 2. Non-ketotic hyperosmolar coma n 3. Skin infections (boils), urinary tract infections and pulmonary infections. Chronic complications 1. Vascular. Ischaemic heart disease, hypertension, cerebrovascular disorders, peripheral vascular disease, gangrene. 2. Renal. Chronic pyelonphritis, recurrent urinary tract infections, K.W. syndrome, papillitis necroticans, renal failure. 3. Neurological. Sensory and motor neuropathy, amyotrophy, autonomic neuropathy. 4. Gastrointestinal system. Dental sepsis, pyorrhoea, gastric distension, diarrhoea with or without steatorrhoea, cholecystitis. 5. Skin. Boils, trophic ulcer of the feet, genital infection, pruritis vulvae. 6. Eye. Retinopathy, changes in refraction requring frequent change in glasses, cataract, glaucoma, eye infections (iritis, iridocyclitis). B7. Respiratory. Pulmonary tuberculosis, bronchopneumonia, pneumonia. 8. Bones and joints. Osteoporosis, neuropathic joint. 9. Genitourinary system. Impotence in men, repeated abortions, miscarriage, stillbirths and big babies in women, hydramnios, toxaemia of pregnancy, intrauterine foetal death, prematurity, congenital anomalies and respiratory distress syndrome.
Management Steps in Diabetic Patients : Type 1 DM: The treatment of type 1 DM is lifelong
insulin replacement. However, alpha glucosidase inhibitors
(acarbose, miglitol) can be given to reduce carbohydrate
absorption.
Diet modifications, physical exercise and education are
also important for the proper control of blood sugar.
Type 2 DM: In obese type 2 patients, weight reduction
should be achieved by diet modification and increased
physical activity. Metformin is the first line therapy in obese
patients. If this is inadequate, sulfonylurea, thiazolidi-
nediones or alpha glucosidase inhibitors are added
alone or in combination. If the combination of these drugs
fails to control blood glucose levels, insulin therapy is
instituted.
Weight maintenance diet is prescribed to non-obese
patients. Sulfonylurea is the first line therapy. If the blood glucose is not controlled by the maximum dose of
sulfonylurea, other agents like biguanide or thiazoli-
dinediones or both are added. If the combination of these
drugs fails, insulin is indicated.
Other indications of insulin in type 2 DM are (a) as a
initial therapy in patients with severe weight loss, (b) patients
with hepatic or renal disease where oral agents are
contraindicated, (c) patients who are acutely ill (DKA, HHS)
and (d) during pregnancy.
Diagnosis :
The diagnosis is made by the measurement of plasma or
capillary blood glucose, which is low.
Treatment : • If the patient is able to swallow, rapidly absorbable
carbohydrates can be administered orally (glucose and
sugar). Alternatively milk, fruit, candy bars, or biscuits
may be given to patients with mild hypoglycemia.
• If the patient is unable to swallow or is in severe
hypoglycemia, intravenous glucose (20-50 ml of 50%
dextrose) is given initially. This is followed by an infusion of 10% dextrose to maintain blood glucose above 100
mg/dL.
• Glucagon injection (1 mg SC or IM) may be given in
severe hypoglycemia if intravenous access can not be
established promptly.
• Prevention of hypoglycemia includes proper education
regarding causes and symptoms of hypoglycemia and
proper adjustment in medication and diet.

Helpful
LikeLiked by 1 person
Thank you ☺️
LikeLike
Good informations👍
LikeLiked by 1 person
Thank you 😊
LikeLike